Contrarian take on GPT-5.6 Sol outperforming physician-written responses and what it means for medical AI adoption
GPT-5.6 Sol, Physician Benchmarks, and the Uncomfortable Truth About Medical Quality
Sam Altman dropped a single line on X that I keep coming back to: “physicians found fewer flaws in GPT-5.6 responses than physician-written responses.” No elaboration. No study link. Just the stat, sitting there.
Most people will scroll past it or frame it as the tired “AI vs. doctors” debate. I think that framing misses the actual point entirely.
What the Data Is Really Telling Us
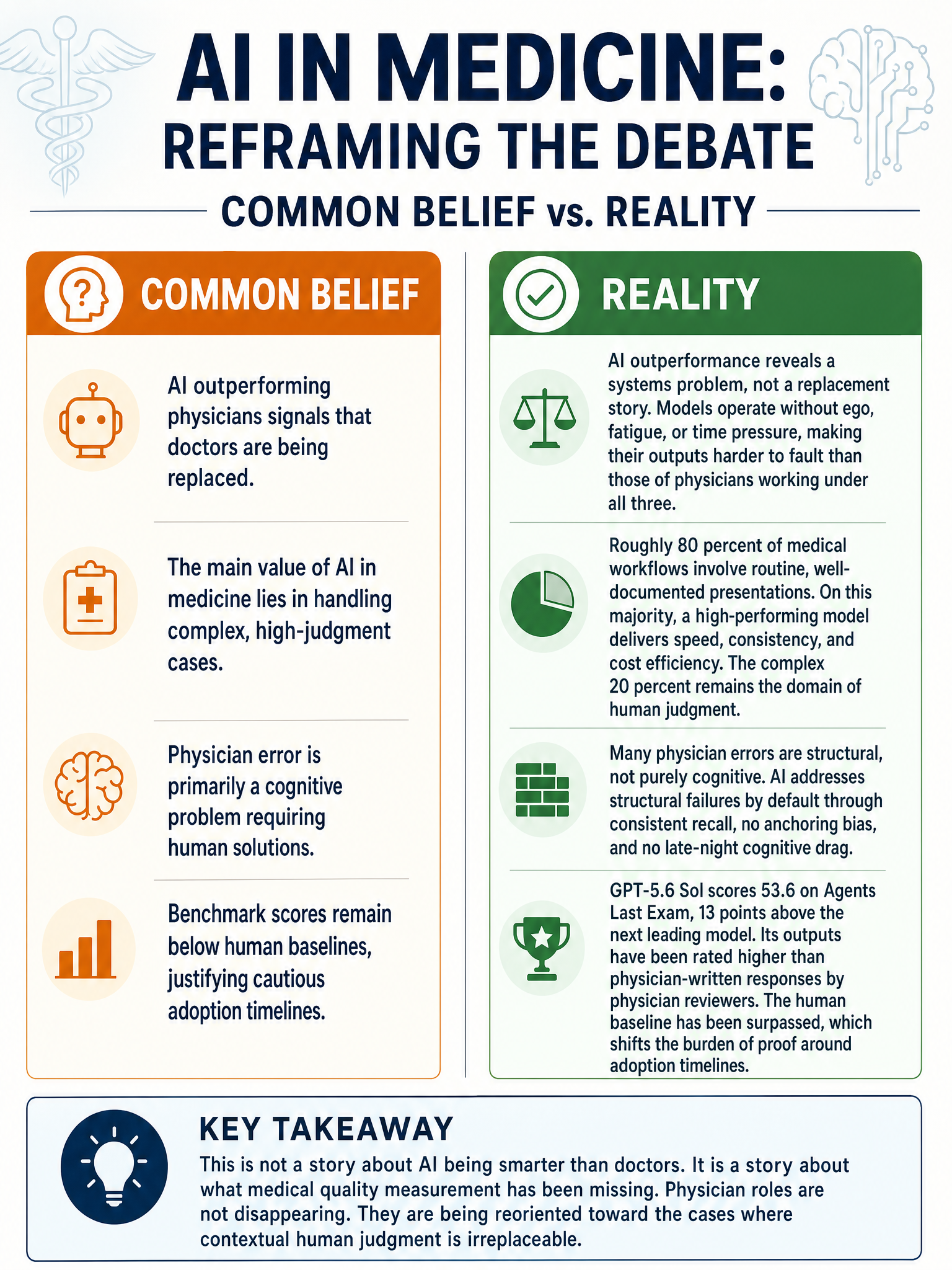
The finding is not that GPT-5.6 Sol is smarter than a physician. It is that physician reviewers, given two sets of responses, found less to criticize in the model’s outputs than in outputs written by their own colleagues.
That is a different claim. And it is a more uncomfortable one.
A physician writing a response is doing so under time pressure, with cognitive load from a full patient schedule, filtered through personal experience that may or may not apply to this specific case. GPT-5.6 Sol has none of those constraints. No fatigue. No ego investment in a prior diagnosis. No clock running.
The question worth sitting with: how much of physician error is actually cognitive error versus structural error? Cognitive errors, the kind that come from bias, fatigue, or heuristic shortcuts, are exactly what a well-trained model does not make. Structural errors, gaps in medical knowledge, failure to recognize a rare presentation, are a different problem. AI has a genuine shot at the first category. The second is still unsolved.
The Systems Problem Nobody Is Talking About
Here is what bothers me about the breathless coverage of this benchmark. The conversation jumps straight to deployment when the real insight is diagnostic.
If a model trained on text is outperforming the written outputs of practicing physicians, that tells you something was already broken in the system producing those physician outputs. It tells you the conditions under which doctors write responses, whether that is asynchronous patient portal messages, referral notes, or discharge summaries, are not conditions optimized for quality.
Medical AI adoption should not be framed as “replace the physician.” It should be framed as “fix the environment the physician is operating in.” The model is a mirror showing us the cost of burning out the humans we rely on.
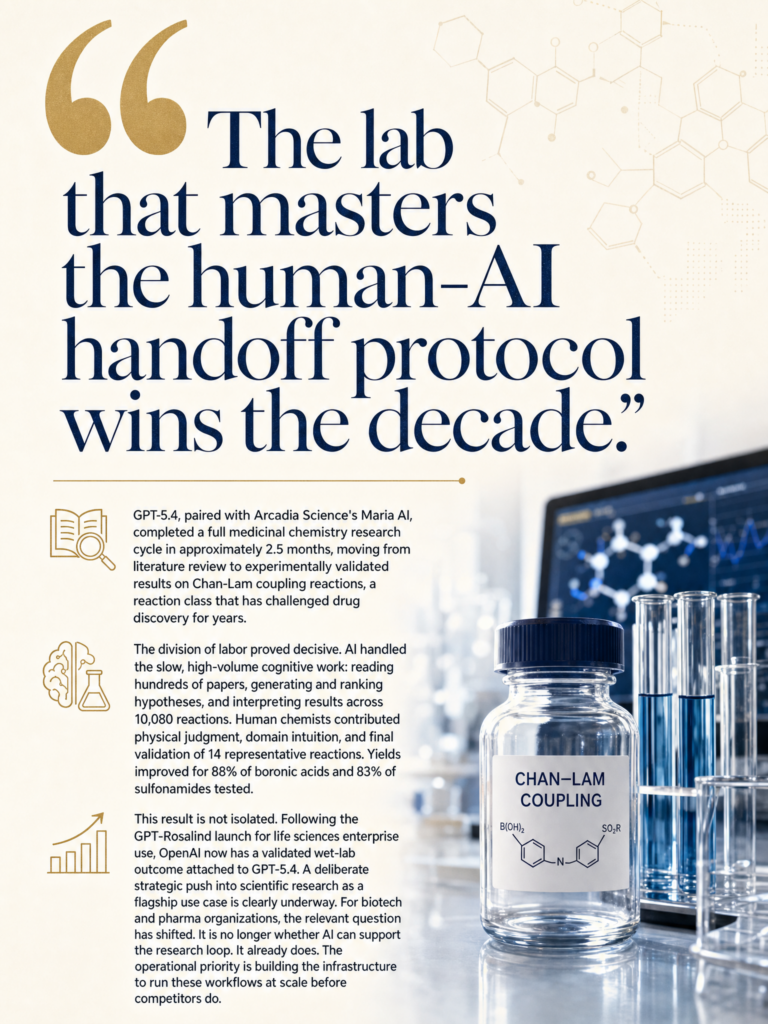
The GPT-5.6 Numbers That Actually Matter
Beyond the medical finding, the raw benchmark data from OpenAI’s release is worth noting. On the Artificial Analysis Coding Agent Index, GPT-5.6 Sol scores 80.0, which is 2.8 points above Claude Fable 5, while using less than half the output tokens and costing roughly one-third less. On Agents’ Last Exam, it hits 53.6, outpacing Claude Fable 5 by 13.1 points at the top reasoning setting.
OpenAI also notes that GPT-5.6 Luna outperforms GPT-5.5 at its highest reasoning setting while costing 25 times less. Altman specifically called out dollars-per-task as the headline metric for enterprises. That framing matters for healthcare. Cost has been a real barrier to clinical AI deployment at scale.
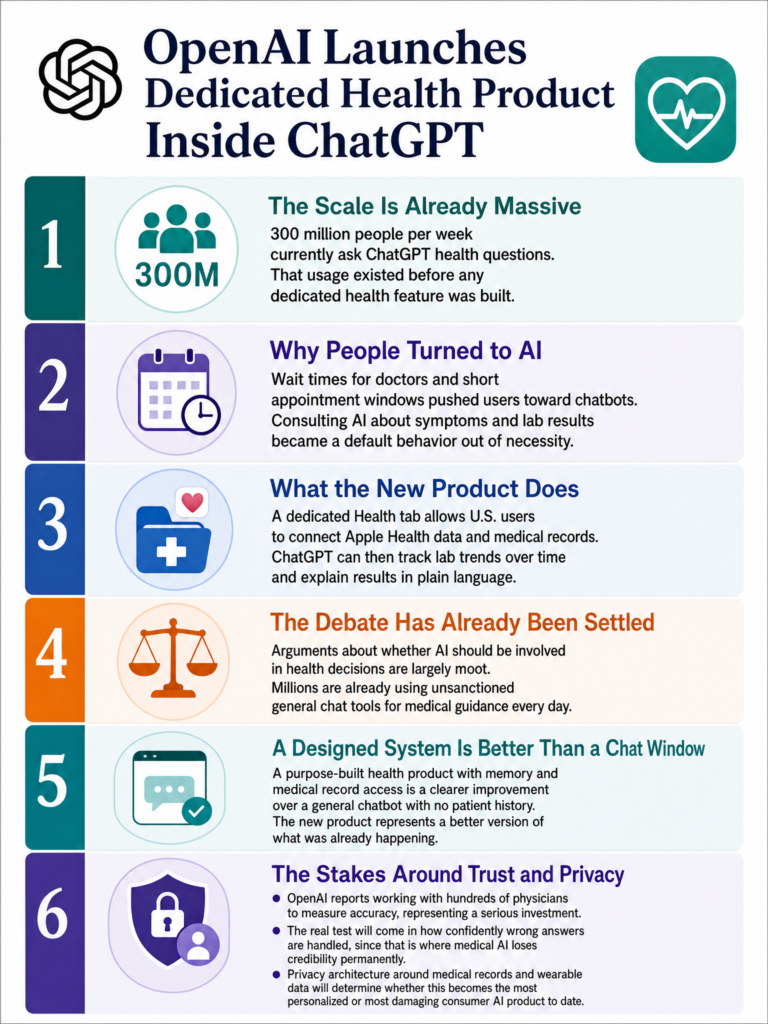
Why Medical AI Adoption Is Still Slow Despite the Numbers
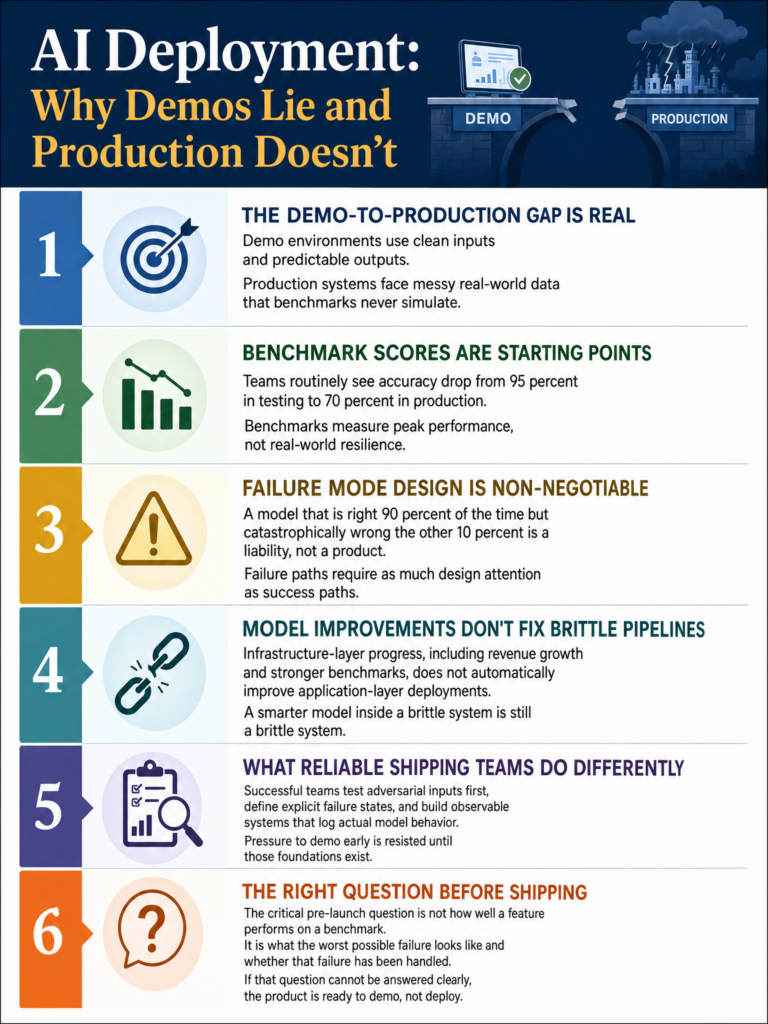
Benchmark performance and clinical deployment are different planets. The regulatory path for AI in clinical decision support is long, the liability questions are unresolved, and physician trust in these systems is, reasonably, still conditional.
But I think a subtler problem is that hospitals and health systems are evaluating AI against an idealized version of physician performance rather than the realistic one. If you benchmark against a physician with eight hours of sleep, a manageable caseload, and thirty minutes per patient, AI does not look as impressive. If you benchmark against actual working conditions in a busy health system, the gap closes fast.
The honest institutional question is whether organizations are ready to admit that the benchmark result implies something about their current working conditions, not just about the AI.
Where This Lands
I am not saying GPT-5.6 Sol should be writing discharge summaries next week. The liability and regulatory infrastructure is not there, and the failure modes for medical AI are genuinely high-stakes.
What I am saying is that a result where physicians find fewer flaws in model outputs than in peer outputs is a signal about systems, not just software. The productive response is not to argue about whether AI can replace doctors. It is to ask why the bar was low enough for the model to clear it, and what that means for how medicine is actually practiced under real conditions.
That is the harder conversation. It is also the more useful one.
Sources
#MedicalAI #GPT56 #AIinHealthcare #ClinicalAI #OpenAI